Health
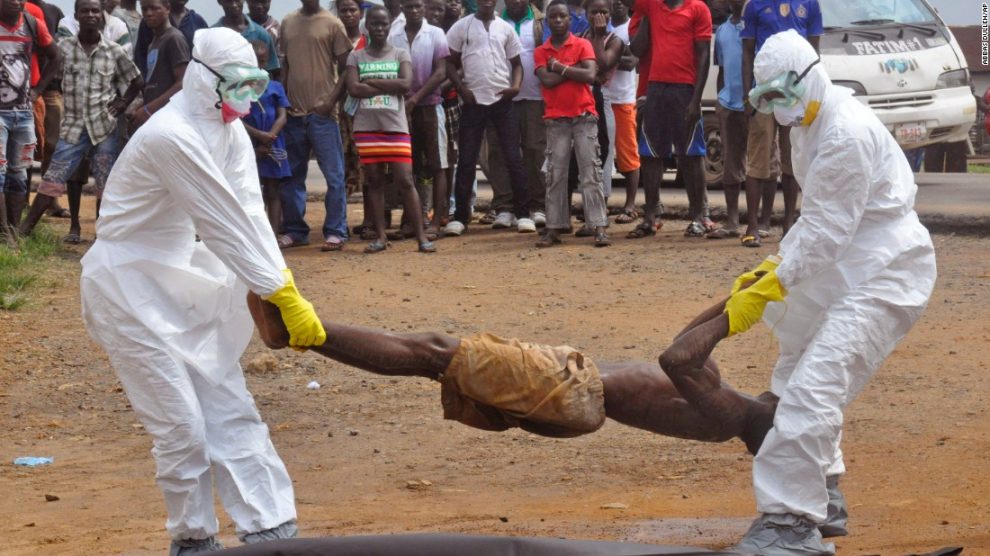
Five Lessons Learned During Latest Ebola Outbreak in DRC

By MSF
Four people died in the most recent Ebola outbreak that occurred in a remote, forested area of the Democratic Republic of Congo (DRC).
This small outbreak (five laboratory-confirmed and three probable cases) was quickly curtailed. The international humanitarian organisation Doctors Without Borders (MSF) shares lessons learned from this first occurrence of the deadly virus since the end of the large-scale Ebola outbreak that devastated West Africa in 2014-2015.
Train frontline health teams
The scale of this outbreak was minimised, thanks in no small part to a nurse named Dieumerci. With a name that literally translates to ‘Thank God’ in French, Dieumerci works at a Ministry of Health centre in northeast DRC, where the first Ebola cases started emerging.
He detected the risk of Ebola in a seriously ill man at the hospital, and rang the alarm. This man turned out to be the second confirmed case during the recent outbreak. Unlike in West Africa prior to the last major outbreak, Ebola is known in the DRC: the Ebola River, where the virus was first discovered, runs 100 kilometres away from where Dieumerci works.
That doesn’t mean that it is common disease in the area, but still, Dieumerci recognised the symptoms. His quick actions should not be taken for granted. Healthcare workers play a crucial role not only for patients, but also for general epidemiological surveillance. However, in many developing countries human resources within the health sector remain starkly inadequate.
On that fateful day where the Ebola patient came to the health centre, Dieumerci could have easily been on a sick leave, or visiting family somewhere else in the country. One cannot rely on a single individual to play the crucial role of on-the-ground surveillance.
What is needed are proper surveillance systems in resource-poor countries, which were clearly lacking in West Africa at the time of the epidemic. So all in all: thank you Dieumerci. We should all hope that during the next outbreak – be it Ebola or any other infectious disease – there will be another Dieumerci to ring the alarm bell for everyone’s sake.
Finally, a forgotten disease is taken seriously
The word “Ebola” doesn’t ring the same after 2014-2015’s devastating epidemic. At least 11,300 people were killed, and over 28,000 were infected. As a result, Dieumerci’s alarm bell sent shock waves across the world. Congolese authorities immediately activated their outbreak response team and had strong support from WHO and other organisations.
Henry Gray, MSF’s project coordinator during this recent outbreak, has worked on seven haemorrhagic fever interventions in DRC, Uganda and West Africa, to name a few. “The pressure we felt was very different from previous comparable outbreaks: it was clearly at the top of the agenda,” he says. “When it comes to Ebola, we have all learned that it’s better to be safe than sorry in order not to repeat the disaster of 2014-2015.
“However, it is sad to still see that other outbreaks in countries do not trigger the same mobilisation, even in regards to the main killer diseases like cholera or measles.
“Once the Ebola outbreak was over, we were able to re-assign some of the MSF staff towards a serious cholera outbreak on the other side of the country. Our teams went on to treat 1,100 cholera patients. “Considering the dire health needs in many parts of the country, additional support is always welcome”.
Old tricks are timeless – back to basics
The promise of new drugs or vaccines should not overshadow the necessity of putting in place the basic pillars of outbreak control.
It all starts with good surveillance, followed by the five pillars of outbreak control:
Safely isolating and treating the sick.
Actively looking for potential new cases and surveilling those who have been in contact with them.
Burying the dead safely.
Engaging and mobilising the affected communities.
Offering psychological support.
In West Africa, the havoc wrecked by Ebola on the entire health system created more indirect than direct victims of the virus: children became prone to infectious diseases because they weren’t vaccinated; Childbirth complications led to the deaths of mothers and/or children because there were no healthcare workers to care for them; untreated cases of malaria became fatal…
International health actors need to do more to support local health facilities that often have much smaller means and equipment: training staff, ensuring there is basic protection equipment available, and that their pharmacies are stocked with first aid supplies and basic medicines. Our experience in DRC has shown that training frontline workers, even when done ad-hoc, can bring sustained effects to improve their performance in surveillance.
Location, location, location
Like the majority of haemorrhagic fever outbreaks prior to West Africa, the recent one occurred in a very remote, forested area.
Here, the virus was already known to exist within an animal reservoir (assumed to be fruit bats) that is occasionally transmitted to apes, monkeys or men. Some people are very mobile in the region, but can only go as far and as fast as their available transportation; which is pretty much nothing beyond walking and the occasional motorbike.
Dieumerci’s village is 45 kilometres from Likati, the closest town. It is home to 18,000 people, with a majestic cathedral and large, but under equipped, hospital serving as remnants of a time when a railroad was still linking plantations across the country. Today that railroad has been eaten by the encroaching jungle. By contrast, in Guéckédou, Guinea – where the West Africa outbreak started – people can jump on a motorbike and be in the heart of the capital Conakry and its 2.5 million people within two days.
These contrasting examples show how isolation from major cities can keep the spread of deadly disease under control.
Medical innovations are not the magic bullet
At the time of the latest outbreak, MSF was willing to use Ebola treatments which were still in development. However this window closed as the outbreak stopped before the process to allow the use of the experimental treatments was complete. However, this event acted as a ‘booster’ – speeding up the process of preparing medical protocols so that new drugs (still in the experimental phase) can be used in ways that are as safe and ethical as possible.
The rVsV-ZEBOV vaccine (the most advanced investigational vaccine candidate for an Ebola outbreak today) is in development, and needs to be implemented through a study protocol. This, and a vaccine strategy – including informed consent under good clinical practice – were mandatory requirements needed from us to access them.
Soon enough, a study protocol was developed and approved by the MSF Ethics Review Board a few months ago. It was ready for implementation should an outbreak occur. Additionally, a dedicated MSF research team was ready to be deployed. Unfortunately, our negotiations at the DRC Ministry of Health level only took place when the outbreak had already been declared.
It took some time for us to explain what we were planning to do, and how this would differ from a vaccination campaign. But, we managed to obtain authorisation from all the regulatory bodies to start activities in case of a future outbreak.
It is likely that the next outbreak (and trust us, there will be a next outbreak) will happen in a similar setting. We can continue to learn how to best tackle it, and ensure that the West Africa Ebola outbreak remains an isolated tragedy.
Since 1990 MSF has responded to over a dozen outbreaks in sub-Saharan Africa. During the devastating Ebola outbreak that struck mainly Liberia, Guinea, and Sierra Leone in 2014-2015, MSF launched one of the largest emergency operations in its 44-year history.
MSF admitted 10,310 patients to its Ebola management centres of which 5,201 were confirmed Ebola cases, representing one-third of all WHO-confirmed cases. During the first five months of the epidemic, MSF handled more than 85 percent of all hospitalized cases in the affected countries.
At the peak of the epidemic, MSF employed nearly 4,300 staff—most of whom were from the affected countries—who ran Ebola management centres, conducted surveillance, contact tracing, and health promotion, and provided psychological support.



By Modupe Gbadeyanka
To expand affordable healthcare in Kenya, Swedfund has invested about $600,000 into Jacaranda Health Limited (Jacaranda Maternity) to support innovations in neonatal intensive care and strengthen Jacaranda’s ability to provide life-saving services to underserved populations.
Jacaranda Maternity provides high-quality maternal health care at more affordable pricing than typical private providers, focusing on women in Nairobi’s low- and middle-income communities.
The new funding will support the opening of new hospitals, upgrading of neonatal care, and improvements to existing facilities.
Maternal and newborn health outcomes in Kenya remain a challenge, with maternal mortality still high despite improvements in skilled birth attendance.
Public health facilities play a central role but face capacity constraints, while access to reliable, quality care varies across regions and income groups.
Private healthcare providers offering essential maternity services at accessible price points can complement public provision.
Jacaranda Maternity aims to expand its network to six hospitals to achieve financial sustainability while scaling its impact. The healthcare provider is a recognised leader in promoting women’s health, with 71 percent of its staff being women, and a track record of effective environmental and social management.
“This investment will help Jacaranda Maternity provide life-saving care to more women and families while furthering Swedfund’s mission to promote inclusive and sustainable healthcare,” a Senior Investment Manager at Swedfund, Audrey Obara, said.

By Adedapo Adesanya
Nigeria will get a $350,000 intervention from the Food and Agriculture Organisation of the United Nations (FAO) to support its response to the ongoing outbreak of Highly Pathogenic Avian Influenza (bird flu) and strengthen the country’s animal health systems.
An agreement was reached on Wednesday during a strategic meeting between the Minister of Livestock Development, Mr Idi Mukhtar Maiha, and the FAO Representative to Nigeria and the Economic Community of West African States, Mr Hussein Gadain, in Abuja.
The intervention, approved under FAO’s Technical Cooperation Programme, will support disease containment efforts in 11 affected states and enhance surveillance, coordination and response mechanisms to prevent further spread of the disease.
Speaking during the meeting, Maiha said effective disease control remains critical to improving livestock productivity and protecting the livelihoods of farmers across the country.
He explained that factors such as drought, scarcity of feed, interaction between livestock and wildlife, as well as cross-border movement of animals have contributed to the spread of diseases in some areas.
“We must continue to strengthen our animal health systems and build the capacity required to respond effectively to disease outbreaks. Our collaboration with FAO will help protect livestock assets, improve productivity and support the broader transformation of the sector,” the minister said.
Mr Gadain commended the federal government’s commitment to the development of the livestock sector and assured that FAO would continue to provide technical support to Nigeria.
He stressed the need to strengthen veterinary services at the state and community levels, improve early detection of diseases and promote biosecurity practices among livestock farmers.
The meeting also reviewed progress on the global campaign to eradicate Peste des Petits Ruminants, a highly contagious disease that affects sheep and goats.
To advance the initiative, the ministry plans to convene a national technical meeting involving veterinary institutions, researchers and practitioners to review Nigeria’s eradication strategy and address gaps in vaccine supply.
As part of preparations, the ministry will engage the National Veterinary Research Institute to assess its vaccine production capacity while exploring other options for vaccine procurement to meet national demand.
Both parties also agreed to accelerate Nigeria’s access to financing under the Pandemic Fund through the One Health approach in collaboration with the Nigeria Centre for Disease Control and the Federal Ministry of Health to strengthen preparedness and response to zoonotic diseases.
Plans are also underway for the Director-General of FAO to participate in the Antimicrobial Resistance Conference scheduled for June 2026 in Abuja, where President Bola Tinubu is expected to be recognised as the African Champion for the eradication of Peste des Petits Ruminants.
The meeting further agreed to inaugurate a Livestock Donor Working Group to coordinate development partner support and advance key initiatives, including the development of a national feed and fodder strategy aimed at improving productivity and sustainability in the livestock sector.

By Aduragbemi Omiyale
A Lagos-based healthcare facility currently in the limelight, Euracare Multi-Specialist Hospital, has faulted the outcome of the investigation panel of the Medical and Dental Council of Nigeria (MDCN) on the death of a 21-month-old Nkanu Nnamdi Esege, son of a renowned author, Chimamanda Ngozi Adichie.
The toddler died some weeks ago after an alleged overdose of sedative propofol, with the family alleging medical negligence.
This week, the panel suspended the two doctors of Euracare, Dr Tosin Majekodunmi and Dr Titus Ogundare.
Reacting to the development in a statement, the hospital claimed it observed “a number of serious concerns that have arisen in the course of these proceedings.”
In the statement made available to Business Post, Euracare emphasised that it vouches for the “professionalism and integrity of our clinical team,” pointing out that “certain established processes and protocols have not been followed in the manner required” during the probe.
While it empathised “with the family of Master Nkanu Nnamdi Esege” over the unfortunate incident, the healthcare firm said there was a “serious breach” by the investigators that “cannot go unaddressed.”
It identified this breach as the disclosure of “matters covered by patient and institutional confidentiality” outside the appropriate channels.
Below is the full statement from Euracare;
Our attention has been drawn to widespread media reports concerning the interim suspension orders and other findings issued by the Medical and Dental Practitioners Investigation Panel against thirteen doctors, two of whom are our clinical staff members in connection with the ongoing proceedings relating to the death of Master Nkanu Nnamdi Esege. We remain fully committed to cooperating with all relevant regulatory and judicial authorities in the course of their inquiries.
We however wish to place on record our confidence in the professionalism and integrity of our clinical team. Dr. Tosin Majekodunmi and Dr. Titus Ogundare who are experienced professionals whose records of service to patients in Nigeria span many years. Both doctors have, in their respective careers, contributed meaningfully to the delivery of quality healthcare to Nigerian patients at a standard comparable to what is obtainable in the world’s leading medical facilities.
In the interest of transparency, since the commencement of this matter, we have conducted a thorough internal review of the clinical events in question, in line with our clinical governance standards and best practices. We have actively demonstrated our commitment to transparency and will continue to engage openly with all inquiries directed at us.
We are also compelled to draw attention to a number of serious concerns that have arisen in the course of these proceedings. It is our position that certain established processes and protocols have not been followed in the manner required. We have further noted, with deep concern, that matters covered by patient and institutional confidentiality appear to have been disclosed outside the appropriate channels, and we consider this a serious breach that cannot go unaddressed.
We wish to state that we stand by the principles of equality, fairness, and good governance. Every party in this matter, including our institution and our staff, is entitled to a process that is conducted with rigour, impartiality, and respect for the rules that govern it. We will be raising these concerns through the appropriate legal and regulatory channels.
We continue to empathize with the family of Master Nkanu Nnamdi Esege. The loss of a child is a grief without measure, and we carry that awareness in everything we say and do in relation to this matter.
-
 Feature/OPED6 years ago
Feature/OPED6 years agoDavos was Different this year
-
Travel/Tourism10 years ago
Lagos Seals Western Lodge Hotel In Ikorodu
-

 Showbiz3 years ago
Showbiz3 years agoEstranged Lover Releases Videos of Empress Njamah Bathing
-
 Banking8 years ago
Banking8 years agoSort Codes of GTBank Branches in Nigeria
-

 Economy3 years ago
Economy3 years agoSubsidy Removal: CNG at N130 Per Litre Cheaper Than Petrol—IPMAN
-

 Banking3 years ago
Banking3 years agoSort Codes of UBA Branches in Nigeria
-

 Banking3 years ago
Banking3 years agoFirst Bank Announces Planned Downtime
-

 Sports3 years ago
Sports3 years agoHighest Paid Nigerian Footballer – How Much Do Nigerian Footballers Earn